
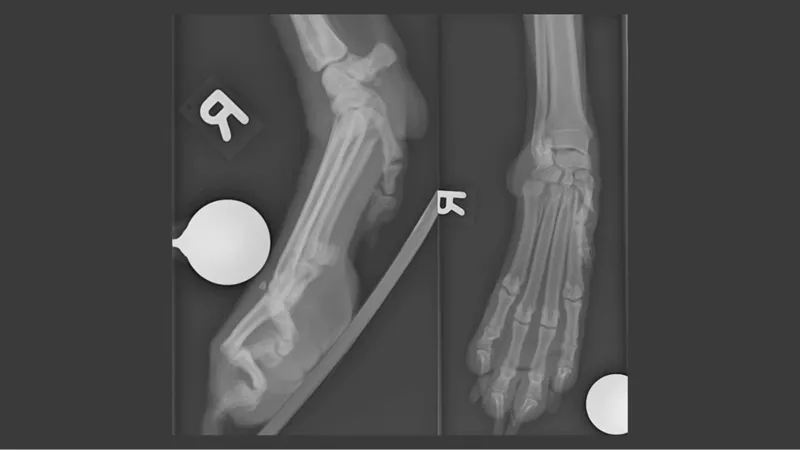
Figure 1: Hyperextension trauma of the carpometacarpal joint.
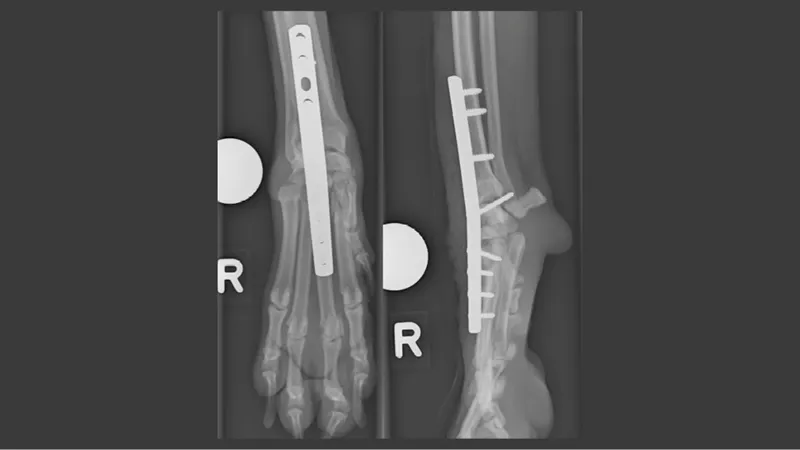
Figure 2: Post-operative control of pancarpal arthrodesis.
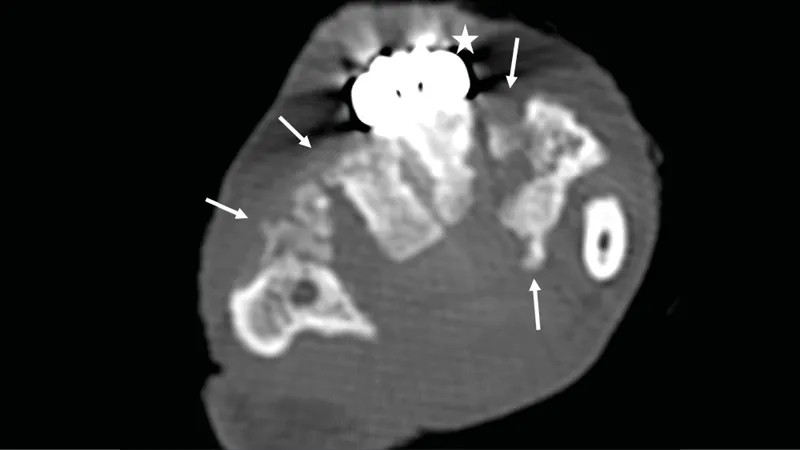
Figure 3: CT control 7 weeks after surgery. Bone formation is visible at several regions of the carpal joint (arrows). The pancarpal arthrodesis plate is located dorsally (star).
Treatment of carpal instability in a dog with pancarpal arthrodesis
An 8-year-old male castrated mix breed dog was referred to the small animal hospital after diagnosis of a carpal instability due to a jump from a 3.5 m height. Initial clinical presentation was stable and orthopedic examination revealed a severe lameness on the right front limb with carpal instability. Stress radiographs confirmed the diagnosis and the suspicion for ligament rupture (Figure 1). In addition to the hyperextension trauma with palmar instability of the carpometacarpal joint, an acute proximal diaphyseal fracture of the metacarpal bone II, carpometacarpal subluxation MC V was visible.
As the dog had severe otitis and dermatitis, those conditions were treated prior to surgical fixation of the carpus with pancarpal arthrodesis, to reduce the risk for an infection. After both dermatological conditions were resolved the dog was operated and pancarpal arthrodesis was performed using a 3.5 mm pancarpal arthrodesis plate. Xcyte, a new osteoinductive material, was additionally introduced into the joint spaces after the cartilage of the carpal articulations was removed with a small burr. Figure 2 shows the post-operative control of the pancarpal arthrodesis on the right front limb.
Bandage changes were performed at the private veterinarian. A small wound was treated with wound management (frequent bandage changes and application of wound coverage). Seven weeks after surgery a control, including a control CT, was performed. The dog showed no lameness. The control CT displayed progressive, but still incomplete carpal ankyloses and persistent dislocated fractures of MC II and V, with little bridging callus.